
How Upper Cervical Chiropractic for Post-Concussion Syndrome Helps the Brain Finally Heal
- New York UCC

- Apr 27
- 7 min read
When most people picture a concussion, they picture the brain. They picture a sudden jolt on a soccer field, a moment of confusion at the bottom of a staircase, a quick visit to a doctor, and a few weeks of rest. What they almost never picture is the neck — and yet some of the most compelling research of the last decade suggests that the upper neck may be one of the most overlooked drivers of why concussion symptoms refuse to go away.
Studies estimate that more than ninety percent of concussive head injuries also produce a meaningful upper cervical injury, because the same rotational and shearing forces that whip the brain around inside the skull also strain the ligaments, joints, and soft tissues at the very top of the spine.

Post-concussion syndrome, often shortened to PCS, is the cluster of symptoms that lingers beyond the typical three- to six-week recovery window. For most people, a concussion resolves on its own. For roughly ten to thirty percent, it does not. The headaches stay. The dizziness stays. The fog, the fatigue, the noise sensitivity, the irritability, the strange feeling that the world is just a little bit off — all of it can stay, sometimes for months and sometimes for years. PCS is more common than the public realizes, and for the people living with it, daily life can shrink dramatically. Driving, screen work, parenting young kids, exercising, holding down a demanding job in New York — anything that involves sustained focus, head movement, or visual stimulation can become exhausting.
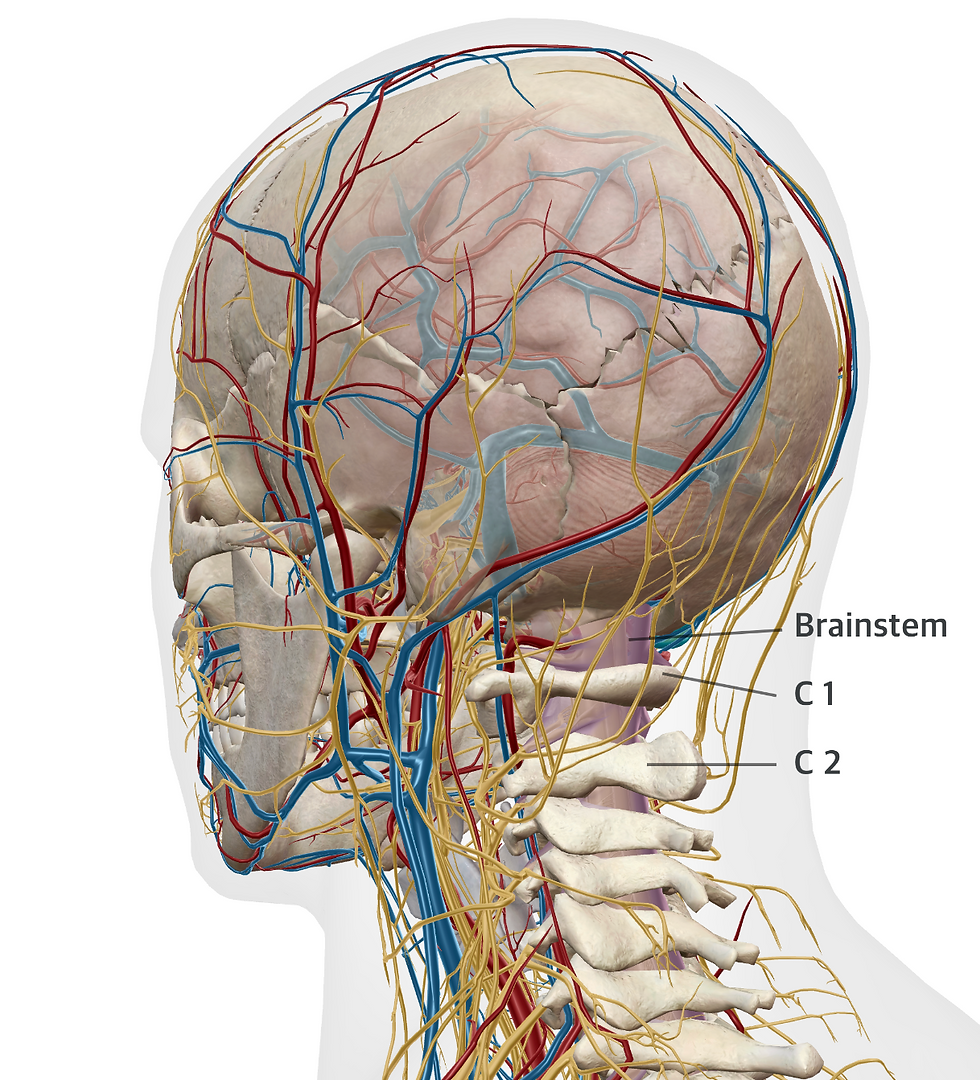
To understand why the upper cervical spine matters so much in this picture, it helps to picture what actually sits there. The atlas, or C1 vertebra, is a small ring-shaped bone that cradles the base of the skull and surrounds the brainstem. The brainstem houses the command centers for blood pressure, heart rate, balance, autonomic regulation, eye movement, and the relay of sensory information between the body and the brain. Below the atlas sits the axis, or C2 vertebra, which contains the dens — a vertical projection that fits up into the atlas like a pivot. Together these two bones make the craniocervical junction, and the CCJ is essentially the most neurologically dense and vascularly delicate intersection in the human body. The vertebral arteries climb through it. Cerebrospinal fluid drains across it. The vagus nerve, the upper cervical nerves, and the trigeminocervical nucleus all converge on it.
When a concussive force whips the head, it almost always shears the ligaments and joint capsules of the CCJ. Even a millimeter of residual misalignment at the atlas can have outsized consequences, because every structure passing through that junction is exquisitely sensitive to position. Misalignment can tighten the small suboccipital muscles that wrap around the brainstem, irritate the trigeminocervical nucleus (which is why concussion headaches so often feel like they originate behind the eyes or at the base of the skull), and disrupt proprioceptive input from the upper neck — input the brain relies on to know where the head is in space. When that proprioception is wrong, the brain receives a mismatch between what the eyes see, what the inner ear feels, and what the neck reports. The result is the dizziness, brain fog, motion sensitivity, and the foggy, unmoored feeling that so many PCS patients describe.
The CCJ also plays a surprising and often-overlooked role in cerebrospinal fluid dynamics. Cerebrospinal fluid bathes the brain and spinal cord, clears metabolic waste through the glymphatic system, and cushions delicate neural tissue. Research using upright MRI has shown that even small misalignments at C1 can alter CSF flow at the foramen magnum, the opening at the base of the skull. After a concussion, when the brain is already working overtime to clear inflammatory byproducts, restricted CSF flow can prolong recovery and amplify symptoms like pressure headaches, light sensitivity, and brain fog. This is one of the lesser-known connections between the upper neck and the post-concussion brain, and it is part of why some patients who have tried everything else find unexpected relief once their atlas alignment is addressed.
Why Upper Cervical Chiropractic for Post-Concussion Syndrome Differs From General Chiropractic
The image many people have of chiropractic care — fast twists, audible cracks, full-spine adjustments — is not what upper cervical care looks like. Techniques like NUCCA, Blair, Atlas Orthogonal, and Knee Chest Upper Cervical use precise, low-force corrections directed only at the atlas and axis. There is no twisting of the neck, no popping, and no cavitation sound. Before any correction is made, three-dimensional imaging — increasingly cone beam computed tomography — is used to map the unique misalignment pattern of that individual patient. The correction is then customized down to fractions of a degree. This precision matters enormously for PCS, because the post-concussion brainstem and ligamentous tissue are still healing and cannot tolerate aggressive manipulation.
Patients who respond well to upper cervical care for post-concussion syndrome often describe the change as something they feel in stages rather than all at once. Sleep tends to improve first. Then the constant background headache softens. Then the dizziness, the visual fatigue, and the brain fog begin to lift, and patients notice they can read, drive, or work on a screen for longer before feeling drained. These improvements line up with what we know about how the CCJ influences brainstem function, autonomic balance, and CSF flow.
Post-concussion recovery is rarely linear, and upper cervical care is rarely the only piece of the puzzle. Vestibular therapy, vision therapy, neuro-optometric rehabilitation, graded sub-symptom exercise, sleep hygiene, and nutritional support all have important roles. The goal of upper cervical care is not to replace these therapies — it is to remove a structural obstacle that often blocks them from working. When the atlas is holding the head off-center, every other rehab intervention is being asked to compensate against a moving target. When the atlas is corrected and held in place, the nervous system finally gets the chance to recalibrate, and the rest of the recovery plan tends to gain real traction.
If you are in New York and have been living with post-concussion symptoms — whether from a sports collision, a slip on the subway stairs, a car accident, a bike crash, or a workplace injury — and you have not yet had your upper cervical spine evaluated, you have not yet tried one of the most mechanistically relevant interventions for your condition. At New York Upper Cervical Chiropractic, we serve patients across NYC and Long Island, as well as commuters from Brooklyn, Queens, the Bronx, Westchester, and northern New Jersey.
Patients searching for an upper cervical chiropractor in New York or post-concussion care in New York will find a precise, gentle, imaging-guided approach. We also work with patients suffering from migraines, vertigo, cervicogenic headaches, TMJ disorder, tinnitus, dysautonomia and POTS, whiplash, Meniere's disease, and chronic neck pain — many of which share the same upper cervical mechanism.
FAQs
Is upper cervical chiropractic safe after a concussion?
Yes — when performed by a properly trained upper cervical specialist using imaging-guided, low-force techniques. There is no twisting or cracking of the neck, and the force used is typically less than what you would feel pressing on a bathroom scale with one finger. We always review imaging and clear medical red flags before any correction.
How long does it take to feel better with upper cervical care for post-concussion syndrome? Every brain heals on its own timeline, but many PCS patients notice improvements in sleep and headache intensity within the first two to four visits, with dizziness, fog, and visual fatigue typically improving over the following weeks to months. Chronic, multi-year PCS cases often require a longer corrective phase but still tend to show steady, measurable progress.
Do I really need imaging before treatment?
Yes — and this is one of the things that sets upper cervical care apart. Because every patient's misalignment pattern is unique, we use precision imaging (often cone beam CT or specialized x-ray series) to calculate a custom correction angle. Treating without that information would be like fitting glasses without a prescription.
New York Upper Cervical Chiropractic
📍 505 Northern Blvd, Suite 309, Great Neck, NY 11021
📞 516) 969-3330
@ drjaewonlee | @newyorkucc
References
Moore J. Chiropractic Management of the Craniocervical Junction in Post-Concussion Syndrome: A Case Series. J Contemp Chiropr. 2019;2(1):92–102.
Marshall CM, Vernon H, Leddy JJ, Baldwin BA. The role of the cervical spine in post-concussion syndrome. Phys Sportsmed. 2015;43(3):274–284. PMID: 26138797.
Cheever K, Kawata K, Tierney R, Galgon A. The Role of Cervical Symptoms in Post-concussion Management: A Systematic Review. Sports Med. 2021;51(9):1875–1891.
Schneider KJ, Meeuwisse WH, Nettel-Aguirre A, Barlow K, Boyd L, Kang J, Emery CA. Cervicovestibular rehabilitation in sport-related concussion: a randomised controlled trial. Br J Sports Med. 2014;48(17):1294–1298.
Leddy JJ, Baker JG, Willer B. Active Rehabilitation of Concussion and Post-concussion Syndrome. Phys Med Rehabil Clin N Am. 2016;27(2):437–454.
Treleaven J. Sensorimotor disturbances in neck disorders affecting postural stability, head and eye movement control. Man Ther. 2008;13(1):2–11.
Steward T. Atlas Subluxation Complex, National Upper Cervical Chiropractic Association Intervention, and Dizziness Improvement: A Narrative Review of Historical Perspectives, Literature Synthesis, and a Path for Future Care. Cureus. 2025 Feb 19 (PMC11927947).
Woodfield HC 3rd, York C, Rochester RP, Bales S, Beebe M, Salminen B, Scholten JN. Craniocervical chiropractic procedures — a précis of upper cervical chiropractic. J Can Chiropr Assoc. 2015;59(2):173–192.
Damadian RV, Chu D. The possible role of cranio-cervical trauma and abnormal CSF hydrodynamics in the genesis of multiple sclerosis. Physiol Chem Phys Med NMR. 2011;41:1–17.
Cassidy JD, Boyle E, Carroll LJ. Population-based, inception cohort study of the incidence, course, and prognosis of mild traumatic brain injury after motor vehicle collisions. Arch Phys Med Rehabil. 2014;95(3 Suppl):S278–S285.
Iverson GL. Outcome from mild traumatic brain injury. Curr Opin Psychiatry. 2005;18(3):301–317.
Trager RJ, Daniels CJ, Hawk C, Taylor DN, Walters SA, Price MR, Anderson KR, Crivelli LS, Mooring SA, Staab CA, Oakley CB. Chiropractic Management of Adults with Cervicogenic or Tension-Type Headaches: Development of a Clinical Practice Guideline. J Integr Complement Med. 2026 (online ahead of print).
Disclaimer: This blog post is for educational purposes only and is not intended as medical advice. Dysautonomia is a complex condition that should be evaluated by a qualified healthcare provider. Upper cervical care may be considered as part of a comprehensive approach. Please consult with your healthcare provider to determine what approach is best for you.


