
Upper Cervical Chiropractic for Trigeminal Neuralgia: What Your Neck Has to Do With "The Suicide Disease"
- New York UCC

- Apr 20
- 8 min read
Trigeminal neuralgia has been called the worst pain known to medicine. People who live with it describe sudden electric shock-like jolts through the face so intense that eating, talking, brushing their teeth, or even feeling a breeze on their cheek can trigger an attack. Some attacks last only a second. Others roll in waves for minutes. Some patients experience hundreds of episodes in a single day.
It is not a rare condition. The National Institute of Neurological Disorders and Stroke estimates that trigeminal neuralgia affects roughly 150,000 people in the United States each year, with women and adults over 50 being most commonly affected. Yet despite how debilitating it is, the underlying cause is often never fully resolved — and most patients spend years cycling through medications, nerve blocks, or surgical procedures without lasting relief.
What most people — and many healthcare providers — don't realize is that the neck, specifically the top two vertebrae of the spine, may play a significant role in triggering or worsening trigeminal neuralgia. Understanding this connection could change the entire trajectory of care for people who are suffering.
What Is Trigeminal Neuralgia, and Why Is It So Severe?
The trigeminal nerve is the fifth cranial nerve, and it is the largest of the twelve cranial nerves. It is responsible for virtually all sensation in the face — touch, pain, temperature, and pressure across the forehead, cheeks, jaw, lips, and teeth. It has three main branches: the ophthalmic (V1), maxillary (V2), and mandibular (V3) divisions, collectively covering the entire face from the scalp to the chin.

When the trigeminal nerve becomes irritated — whether from compression, inflammation, or demyelination — the signals it sends to the brain become chaotic. Normally harmless stimuli, like a gust of wind or taking a sip of water, get misinterpreted as catastrophic pain. The neurological mechanism is similar to what happens when a frayed electrical wire sparks at the slightest touch. The brain can't distinguish between "light breeze" and "severe injury," so it responds with maximum alarm. That alarm is the searing, lightning-bolt pain that patients describe.
The most commonly discussed explanation for trigeminal neuralgia involves vascular compression—where a nearby blood vessel, often the superior cerebellar artery, comes into contact with the trigeminal nerve near the brainstem. Over time, this contact may affect the protective myelin sheath surrounding the nerve, which can contribute to abnormal nerve signaling.
At the same time, vascular compression may not be the only factor involved. In many cases, there can be additional or contributing influences that are important to consider when evaluating and managing this condition.
The Surprising Link Between Trigeminal Neuralgia and the Craniocervical Junction
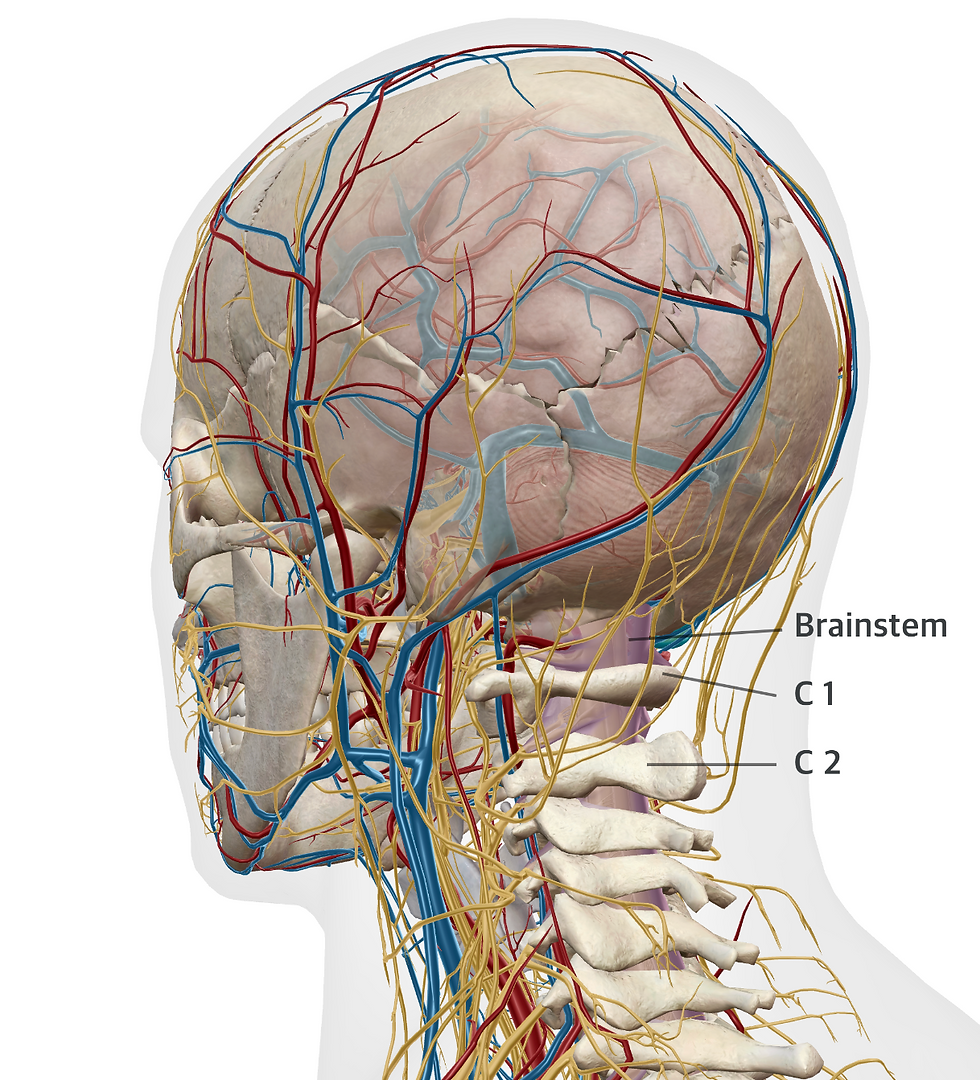
Here is what most patients are never told: the trigeminal nerve does not begin and end cleanly at the brainstem. Its sensory nucleus — the structure that processes all the incoming facial pain signals — extends downward through the brainstem and all the way into the upper cervical spinal cord, reaching as far as C2 and sometimes C3. This elongated structure is called the trigeminal nucleus caudalis (TNC), and its location means it sits in direct anatomical proximity to the atlas (C1) and axis (C2) vertebrae.
This is the lesser-known connection that is crucial to understand. The upper two vertebrae of the spine — the atlas and axis — form what is called the craniocervical junction (CCJ). This is one of the most mechanically complex and neurologically dense regions of the human body. The brainstem, the beginnings of the spinal cord, twelve cranial nerve pathways, major arteries supplying the brain, and the cerebrospinal fluid (CSF) drainage pathways all converge in this tight space.
When the atlas misaligns — even by fractions of a millimeter — it can create mechanical tension, inflammation, and altered neurological signaling in the very structures that neighbor the trigeminal nucleus caudalis. A misaligned atlas can compress the dura mater (the protective membrane surrounding the spinal cord and brain), restrict CSF flow, alter blood flow through the vertebral arteries, and place stress on the brainstem itself. All of these disruptions can potentially sensitize or irritate the trigeminal pathways, contributing to the misfiring that produces facial pain.
A 2020 paper published in the Journal of Contemporary Chiropractic examined the craniocervical posture hypothesis for trigeminal neuralgia and found that most TN patients could provoke facial pain through neck flexion — suggesting that mechanical forces at the cervicogenic level directly influence trigeminal nerve behavior. This is not a minor detail. It is a strong mechanistic clue that the position of the upper cervical spine matters deeply in this condition.
How Does an Atlas Misalignment Develop?
The atlas and axis are the only vertebrae in the spine that can move as independently as they do. The atlas supports the entire weight of the head — typically 10 to 12 pounds — and allows it to nod and rotate. Because of this unique design, the atlas has no interlocking disc above it and relies heavily on soft tissue structures (ligaments, muscles, fasciae) for stability.

This makes the atlas particularly vulnerable to misalignment following trauma. Whiplash from a car accident, a fall, a sports injury, even a difficult birth can shift the atlas out of its optimal position. Repetitive postural stress — years of forward head posture from desk work or screens — can also gradually shift the alignment of the upper cervical spine. In many cases, patients with trigeminal neuralgia have a history of head or neck trauma years or even decades before their facial pain began.
The atlas does not have to be dramatically out of place to cause problems. Even subtle misalignments can alter the biomechanical forces across the brainstem, change the tension in the spinal dura, and disrupt the fluid dynamics that keep cranial nerve tissue healthy. Small shifts can have outsized neurological consequences in this region.
What Upper Cervical Chiropractic Care for Trigeminal Neuralgia Looks Like
Upper cervical chiropractic care focuses exclusively on this critical region at the top of the spine. Unlike conventional chiropractic adjustments that treat the whole spine with general manipulation, upper cervical care is a highly specialized approach that uses precise imaging — often including cone beam CT (CBCT) or three-dimensional X-rays — to analyze the exact degree and direction of atlas misalignment. The adjustment itself is gentle and specific, with no twisting, cracking, or forceful thrusting of the neck.

At New York Upper Cervical Chiropractic, every patient undergoes a detailed neurological and structural evaluation before any adjustment is made. The goal is to understand exactly how that individual's atlas has shifted, what structures may be under stress, and how a precise correction can restore normal alignment and allow the nervous system to function without interference.
A 2023 case series published in ScienceDirect examined five patients with chronic, severe daily trigeminal neuralgia who received Upper Cervical Chiropractic adjustments over eight weeks. Two participants reported complete cessation of their trigeminal neuralgia. Two others experienced a significant reduction in pain. Three of the five reduced their medication dosage during the study period. While this is a small study, it represents meaningful clinical evidence that upper cervical care can be a valuable tool in managing this otherwise difficult condition.
An earlier case report in a peer-reviewed journal followed a 68-year-old woman with more than seven years of worsening trigeminal neuralgia following brain tumor resection. After years of failed medical management, she found satisfactory improvement through chiropractic care targeting the upper cervical spine and soft tissue structures.
The Daily Reality of Living With Trigeminal Neuralgia
For those who haven't experienced it, the impact of trigeminal neuralgia on daily life is almost impossible to fully comprehend. Simple acts become terrifying. Patients avoid eating in public because chewing might trigger an attack. They stop smiling. They don't brush certain teeth. They avoid wind, cold air, dental work, and conversations. Many develop anxiety and social withdrawal. Depression is common. The condition's historical nickname — "the suicide disease" — reflects how many patients historically found the pain intolerable before modern treatments existed.
Even with today's most effective medications, many patients experience only partial relief, and the drugs often come with side effects including dizziness, cognitive dulling, and liver stress. Long-term medication use is not a neutral intervention, and many patients desperately want a solution that addresses the source of the problem rather than just dampening the signal.
That is precisely why a structural approach that examines and corrects the atlas and axis — the vertebrae sitting millimeters from the trigeminal nucleus caudalis — deserves serious attention.
Upper Cervical Chiropractic for Trigeminal Neuralgia: Finding Care in New York
If you or someone you love is living with the relentless facial pain of trigeminal neuralgia in New York, you deserve a thorough evaluation that looks at every possible contributing factor — including the alignment of your upper cervical spine. Our practice, New York Upper Cervical Chiropractic, is located in Great Neck and serves patients from Queens, Brooklyn, Bronx, and Long Island.
Many of our patients have already seen neurologists, tried multiple medications, and even explored surgical options before discovering upper cervical care. For them, finally understanding the anatomical connection between their atlas alignment and their trigeminal pain is a revelation. If you've been searching for an "upper cervical chiropractor in New York," or a natural approach to facial nerve pain and trigeminal neuralgia in Manhattan, we'd love to speak with you.
We also work with patients experiencing related conditions — including cervicogenic headaches, migraines, vertigo, tinnitus, Meniere's disease, post-concussion syndrome, TMJ disorder, occipital neuralgia, and autonomic nervous system dysfunction — all of which share the same anatomical origin point at the craniocervical junction. A free consultation is available, and it begins with a conversation, not a commitment.
References
Barker, F.G., Jannetta, P.J., et al. (1996). The long-term outcome of microvascular decompression for trigeminal neuralgia. New England Journal of Medicine, 334(17), 1077–1083.
Obermann, M. (2010). Treatment options in trigeminal neuralgia. Therapeutic Advances in Neurological Disorders, 3(2), 107–115.
Zakrzewska, J.M., & Linskey, M.E. (2014). Trigeminal neuralgia. BMJ, 348, g474.
Goadsby, P.J., & Raskin, N.H. (2008). Headache. In Harrison's Principles of Internal Medicine (17th ed.). McGraw-Hill.
Smith, D.L., et al. (2023). Atlas orthogonal chiropractic management of trigeminal neuralgia: A series of case reports. Journal of Chiropractic Medicine (published via ScienceDirect).
Doursounian, L., et al. (2020). Is one cause of trigeminal neuralgia subluxation of craniocervical posture? Journal of Contemporary Chiropractic, 3(1).
Rix, G.D., & Metcalfe, A. (2010). Trigeminal neuralgia and chiropractic care: a case report. Journal of the Canadian Chiropractic Association, PMC2921783.
Devor, M., Amir, R., & Rappaport, Z.H. (2002). Pathophysiology of trigeminal neuralgia: the ignition hypothesis. The Clinical Journal of Pain, 18(1), 4–13.
Love, S., & Coakham, H.B. (2001). Trigeminal neuralgia: pathology and pathogenesis. Brain, 124(Pt 12), 2347–2360.
National Institute of Neurological Disorders and Stroke. (2023). Trigeminal Neuralgia Fact Sheet. NIH Publication.
Bogduk, N. (1992). The anatomical basis for cervicogenic headache. Journal of Manipulative and Physiological Therapeutics, 15(1), 67–70.
Rosa, S., et al. (2017). Upper cervical chiropractic care and the autonomic nervous system: clinical relevance and emerging evidence. Annals of Vertebral Subluxation Research, 2017(1), 1–10.


